
What is Haematuria?
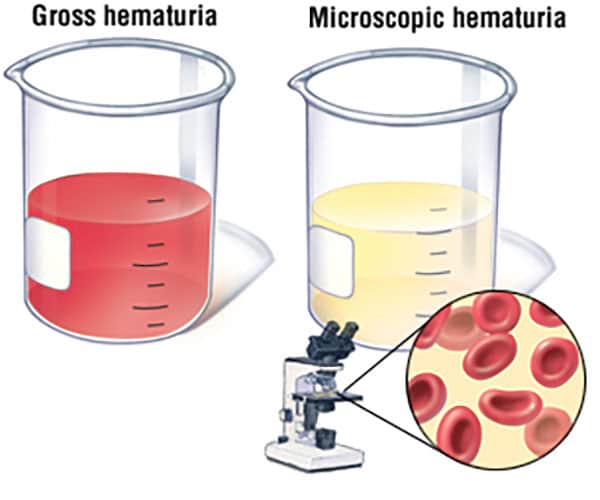
Haematuria is defined as the presence of blood in the urine. Depending on the amount of blood present haematuria can be:
Gross i.e. visible with the naked eye. The urine may be red or cola coloured and in severe cases blood clots may be present which can block the passage of urine.
Microscopic where on only traces of blood are present which can only be detected by microscopic examination of the urine or using a dipstick
Haematuria, must be taken seriously and investigated, as occasionally it can be due to a cancerous cause.
What are the causes of the Haematuria?
Some benign causes are:
- Urinary tract infections.
- Urinary tract stones.
- Benign enlargement of the prostate (BPH).
- Prostatitis (inflammation of the prostate).
- Glomerulonephritis (inflammation in the kidney).
- Trauma.
- Recent bladder procedure or instrumentation.
- Urinary tract damage either from blunt or sharp trauma.
- Non-infective cystitis (inflammation of the bladder).
- Radiation cystitis.
- Haemorrhagic cystitis (can be caused by certain medications like cyclophosphamide).
- Urethritis (inflammation of the urethra or the tube that empties the bladder to the outside).
Malignant (cancerous) causes are:
- Bladder cancer.
- Kidney cancer.
- Prostate cancer – although haematuria is not a common presentation.
Certain blood-thinning medications (e.g. warfarin) can precipitate blood in the urine. In this situation, the underlying cause of the bleeding would still need to be looked for.
What can be mistaken for Haematuria?
- Menstruation – the bleeding from a period can sometimes be mixed in with urine and be confused as haematuria.
- Rectal bleeding – bleeding from the rectum can drip into the toilet bowl and get mixed in with urine.
- Heavy exercise or physical exertion can cause myoglobinuria (muscle breakdown product in the urine) and cause the urine to appear red or brown in colour.
- Medications that cause red urine:
- Antibiotics like nitrofurantoin, sulfamethoxazole.
- Anti-tuberculosis drugs (rifampicin).
- Parkinson’s drugs (levodopa, methyldopa).
- Food that turn urine red, including beetroot, rhubarb and blackberries.
How is Haematuria investigated?
Urine tests
A mid stream urine sample is sent for microscopy, and cultured for bacteria (infection). If any bacteria are grown they are tested for susceptibility to different antibiotics. The microscopy can also tell the shape of the red blood cells and infer whether they originate from the kidney or lower down the urinary tract (e.g. bladder). Microscopy can also look for cancer cells (cytology) and 3 urine samples are collected over consecutive days for this test.
Blood tests
A full blood count is done to check how much blood the patient has lost and whether a blood transfusion is needed. Other blood tests look at kidney function, calcium levels (if there is a kidney stone), blood electrolyte levels and blood clotting tests.
Radiological imaging
Ultrasound or CT scan to look for signs of infection, stones, kidney obstruction, cancer and anatomical abnormalities.
Cystoscopy
Cystoscopy is examination of the inside of the bladder and urethra with a special telescope. A Cystoscopy examination may be recommended. It is important to note that an Ultrasound or a CT scan cannot accurately pick up bladder wall abnormalities such as a bladder tumour.
How is Haematuria treated?
Treatments for haematuria vary widely depending on the underlying cause. It is impossible to say what, if any, treatment will be needed until a cause is found.
What if no cause is found?
Quite often, no obvious cause for haematuria is found. A complete workup effectively rules out the serious causes for blood in the urine (for example, cancer), so it is appropriate to just keep things under review. If the haematuria recurs or increases in severity, the investigations may need to be repeated, or additional specialised tests may be need to be performed, to be sure there is no serious underlying problem.
Disclaimer
This information is intended as a general educational guide and may not apply to your situation. You must not rely on this information as an alternative to consultation with your urologist or other health professional.
Not all potential complications are listed, and you must talk to your urologist about the complications specific to your situation.